

On this page:
About LGSOC
Key distinctions
LGSOC affects younger patients
Median age at diagnosis is 55.5 years;3 patients have been treated as young as 19 and as old as 79.4
It is less sensitive to chemotherapy
Often responds poorly to chemotherapy compared with high-grade serous ovarian cancer (HGSOC).5
Nonspecific signs and symptoms of ovarian cancer
Symptoms generally overlap with other subtypes of ovarian cancer, other gynecologic and GI cancers, and several benign conditions.6,7 LGSOC symptoms include6,8:
- Bloating
- Pelvic or abdominal pain
- Trouble eating or feeling full quickly
- Urinary symptoms of frequency or constant sense of having to urinate
- Fatigue
- Upset stomach
- Back pain
- Changes in period patterns such as heavier bleeding or irregular bleeding
Key stats
~80%
of patients are diagnosed at an advanced stage1
Over 80%
of patients will experience a relapse1
Less than 5-10%
of all serous ovarian cancers are LGSOC9
~90 months
median overall survival (OS)10
~1,000-2,000
new cases are diagnosed in the US each year11
Patients with LGSOC have poor response rates (0-15%) to chemotherapy in the recurrent setting and are at high risk for recurrence.12,13
Clinically unique
How is LGSOC different from HGSOC?
LGSOC is clinically, histologically, and molecularly distinct from high-grade serous ovarian cancer (HGSOC).14 HGSOC and LGSOC are distinguished with a two-tiered pathology grading system based primarily on the assessment of nuclear atypia with the mitotic index used as a secondary feature.15
In contrast to HGSOC, LGSOC is characterized by an indolent clinical course with a relatively higher resistance (0%-15% response rate in the recurrent setting) to chemotherapy5,12,13 and a high rate (over 80%) of relapse.1
Although LGSOC is associated with prolonged survival compared to HGSOC, quality of life is an important issue, and patients may undergo prolonged ineffective treatments. 10,16
The histomorphologic features of LGSOC are characterized by low-grade (mild-to-moderate) nuclear atypia and low mitotic activity.15 At the molecular level, LGSOC do not harbor TP53 mutations and often exhibit RAS/MAPK pathway alterations.17,18
While once thought to be on a continuum with high-grade serous ovarian carcinoma (HGSOC), LGSOC is now recognized as its own subtype of ovarian cancer, with distinctly different characteristics from HGSOC.3 LGSOC behaves differently than HGSOC in both clinical course and overall prognosis.3 Effective management depends on its differentiation from HGSOC.10
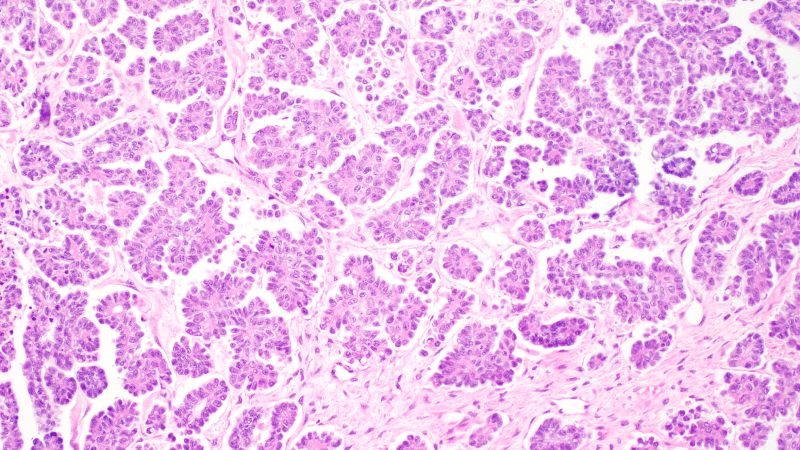
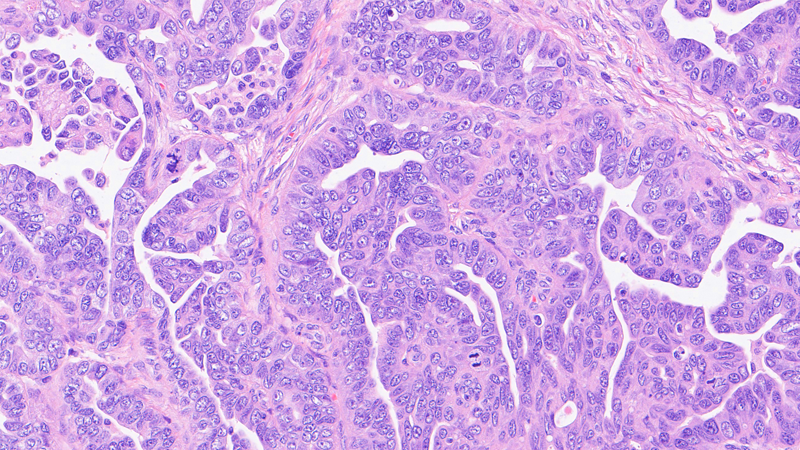
Move the slider from right to left to view histological features of HGSOCs and LGSOCs.
High-grade serous cancer is characterized by marked nuclear pleomorphism and abundant mitotic features. Low-grade serous cancer shows mild nuclear atypia.15
A closer look
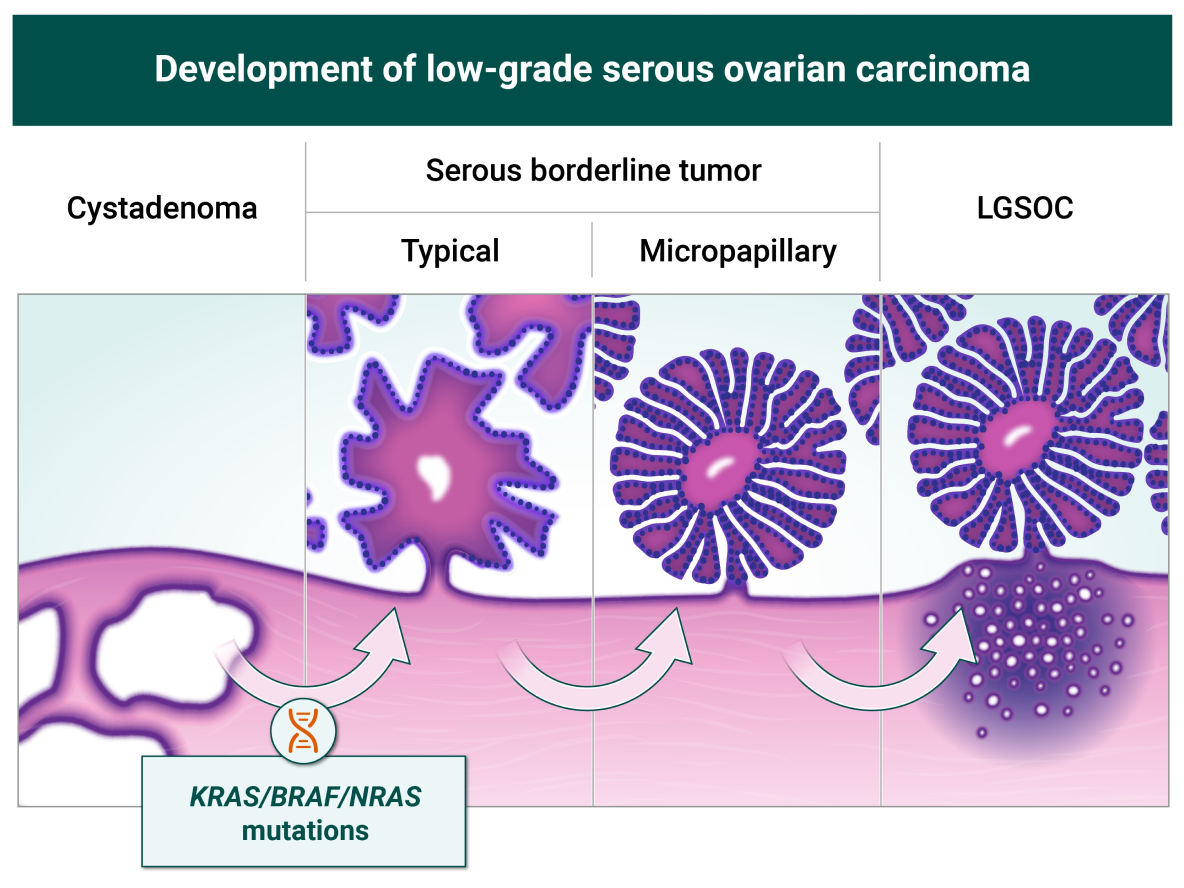
The pathogenesis of LGSOC
Apart from estrogen-related signaling, the mitogen-activated protein kinase (RAS/MAPK) pathway plays a prominent role in the pathogenesis of LGSOC, present in ~60% of LGSOC.17,19 LGSOC may arise from serous borderline tumors (SBT) or as a de novo malignancy from the ovary or peritoneum.20 Alterations affecting the MAPK pathway are most commonly somatic KRAS (33%), NRAS (11%), and BRAF (11%).17
LGSOC in action
Mechanism of disease
Younger patients, advanced disease, few options
Unmet need in LGSOC
With no FDA-approved drugs or treatments specifically for LGSOC,2 there is a high unmet need for patients diagnosed with this rare form of ovarian cancer. These characteristics of LGSOC highlight the urgency of the unmet need:

Advanced stage at diagnosis
Because signs and symptoms are nonspecific to LGSOC,6 patients may be misdiagnosed, and accurate diagnosis of LGSOC can be significantly delayed.10 In fact, ~80% patients receive their diagnosis at advanced stages of LGSOC (stages II-IV).1

Younger patients
Compared to HGSOC, LGSOC is often diagnosed in younger women. Median age at diagnosis is 55.5 years (19-79 years) vs 63 with HGSOC.3 Quality of life is an important issue, and patients may undergo prolonged ineffective treatments.5,16,21

Current treatment regimens
Because there are no FDA-approved treatments for LGSOC,2 the primary treatment method is surgery when possible in both newly diagnosed and recurrent LGSOC.22 Patients may be treated with chemotherapy alone or along with hormone therapy.12 However, LGSOC has substantially lower sensitivity to chemotherapy than HGSOC,5 and hormone therapy is not well studied in LGSOC.12 Recurrence rates with current regimens are high in LGSOC; in over 80% of patients, cancer will relapse.1

Limited treatment options
Recurrent disease has limited treatment options, including: secondary cytoreduction,22 clinical trials, chemotherapy, endocrine therapy, or targeted therapies.17,23
Hear from experts
Considerations when treating younger women with LGSOC
Without FDA-approved, targeted treatments for LGSOC,2 patients and HCPs may be unsure about the best next steps.
- Babaier A, Mal H, Alselwi W, Ghatage P. Low-grade serous carcinoma of the ovary: the current status. Diagnostics (Basel). 2022;12(2):458. doi:10.3390/diagnostics12020458
- Banerjee SN, Ring KL, Nieuwenhuysen EV, et al. Initial efficacy and safety results from ENGOT-ov60/GOG-3052/RAMP 201: a phase 2 study of avutometinib (VS-6766) 6 defactinib in recurrent low-grade serous ovarian cancer (LGSOC). J Clin Oncol. 41. No 16_suppl (June 1, 2023) 5515-5515
- Plaxe SC. Epidemiology of low-grade serous ovarian cancer. Am J Obstet Gynecol. 2008;198(4):459.e1-8; discussion 459.e8-9 doi:10.1016/j.ajog.2008.01.035
- Okoye E, Euscher ED, Malpica A. Ovarian low-grade serous carcinoma: a clinicopathologic study of 33 cases with primary surgery performed at a single institution. Am J Surg Pathol. 2016;40(5):627-635. doi:10.1097/PAS.0000000000000615
- Grabowski JP, Harter P, Heitz F, et al. Operability and chemotherapy responsiveness in advanced low-grade serous ovarian cancer. An analysis of the AGO Study Group metadatabase. Gynecol Oncol. 2016;140:457-462. doi:10.1016/j.ygyno.2016.01.022
- Harvard Health. Certain symptoms may be early signs of ovarian cancer. January 20, 2017. Accessed August 7, 2023. https://www.health.harvard.edu/cancer/certain-symptoms-may-be-early-signs-of-ovarian-cancer
- Ricciardi E, Baert T, Ataseven B, et al. Low-grade serous ovarian carcinoma. GebFra Science. 2018;78:972-976.
- Ferrell B, Smith S, Cullinane C, Melancon C. Symptom concerns of women with ovarian cancer. J Pain Symptom Manage. 2003;25(6):528-538. doi:10.1016/s0885-3924(03)00148-9
- Matsuo K, Machida H, Grubbs B, et al. Trends of low-grade serous ovarian carcinoma in the United States. J Gynecol Oncol. 2018;29(1):e15. doi:10.3802/jgo.2018.29.e15
- Gockley A, Melamed A, Bregar AJ, et al. Outcomes of women with high-grade and low-grade advanced-stage serous epithelial ovarian cancer. Obstet Gynecol. 2017;129:439-447. doi:10.1097/AOG.0000000000001867
- Verastem Oncology. Let’s talk about LGSOC. Accessed August 9, 2023. https://letstalkaboutlgsoc-hcp.com/
- Gershenson DM. Trametinib versus standard of care in patients with recurrent low-grade serous ovarian cancer (GOG 281/LOGS): an international, randomised, open-label, multicentre, phase 2/3 trial. Lancet. 2022;399(10324):541-553. doi:10.1016/S0140-6736(21)02175-9
- Monk JB. MILO/ENGOT-ov11: Binimetinib versus physician’s choice chemotherapy in Recurrent or Persistent Low-Grade Serous Carcinomas of the Ovary, Fallopian Tube, or Primary Peritoneum. J Clin Oncol. 2020;38(32):3753-3762. doi:10.1200/JCO.20.01164
- Vang R, Shih IeM, Kurman RJ. Ovarian low-grade and high-grade serous carcinoma: pathogenesis, clinicopathologic and molecular biologic features, and diagnostic problems. Adv Anat Pathol. 2009;16(5):267-282. doi:10.1097/PAP.0b013e3181b4fffa
- Malpica A, Deavers MT, Lu K, et al. Grading ovarian serous carcinoma using a two-tier system. Am J Surg Pathol. 2004;28(4):496-504. doi:10.1097/00000478-200404000-00009
- Grisham RN, Slomovitz BM, Andrews N, et al. Low-grade serous ovarian cancer: expert consensus report on the state of the science. Published online August 17, 2023. Int J Gynecol Cancer. 2023;33(9):1331-1344. doi:10.1136/ijgc-2023-004610
- Manning-Geist B, Gordhandas S, Liu YL, et al. MAPK pathway genetic alterations are associated with prolonged overall survival in low-grade serous ovarian carcinoma. Clin Cancer Res. 2022;28:4456-4465. doi:10.1158/1078-0432.CCR-21-4183
- Wong KK, Tsang YTM, Deavers MT, et al. BRAF mutation is rare in advanced-stage low-grade ovarian serous carcinomas. Am J Pathol. 2010;177(4):1611-1617. doi:10.2353/ajpath.2010.100212
- ElNaggar A, Robins D, Baca Y, et al. Genomic profiling in low grade serous ovarian cancer: identification of novel markers for disease diagnosis and therapy. Gynecol Oncol. 2022;167(2):306-313. doi:10.1016/j.ygyno.2022.09.022
- Shvartsman HS, Sun CC, Bodurka DC, et al. Comparison of the clinical behavior of newly diagnosed stages II-IV low-grade serous carcinoma of the ovary with that of serous ovarian tumors of low malignant potential that recur as low-grade serous carcinoma. Gynecol Oncol. 2007;105(3):625-629. doi:10.1016/j.ygyno.2007.01.030
- Schmeler KM, Sun CC, Bodurka DC, et al. Neoadjuvant chemotherapy for low-grade serous carcinoma of the ovary or peritoneum. Gynecol Oncol. 2008;108:510-514. doi:10.1016/j.ygyno.2007.11.013
- Crane EK, Sun CC, Ramirez PT, et al. The role of secondary cytoreduction in low-grade serous ovarian cancer or peritoneal cancer. Gynecol Oncol. 2015;136(1):25-29. doi:10.1016/j.ygyno.2014.11.005
- Armstrong DK, Alvarez RD, Backes FJ, et al. NCCN Guidelines® Insights: Ovarian Cancer, Version 3.2022. J Natl Compr Canc Netw. 2022;20(9):972-980. doi:10.6004/jnccn.2022.0047